Medical Reimbursement Consultants since 1985, 903 343-2454

2023 E&M Changes Full 1 Hour Webinar
2023 brings the 2021 E&M rules to ALL PLACES OF SERVICE. This means the 95/97 rules are thrown out the window, along with the deletion of certain codes. This is great news and should save medical providers a ton of time.
This Non-CEU version of the webinar will cover the new coding rules. This includes:
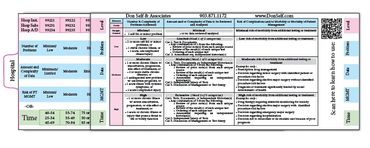
How to select the level of service based on MDM or Time
What code sets were deleted
The prolonged service codes that were added
Examples of how to determine MDM elements
and more...
Photo Gallery